

You are now leaving the aHUSSource.com website.
Alexion is not responsible for content included on third-party websites. Do you want to proceed?

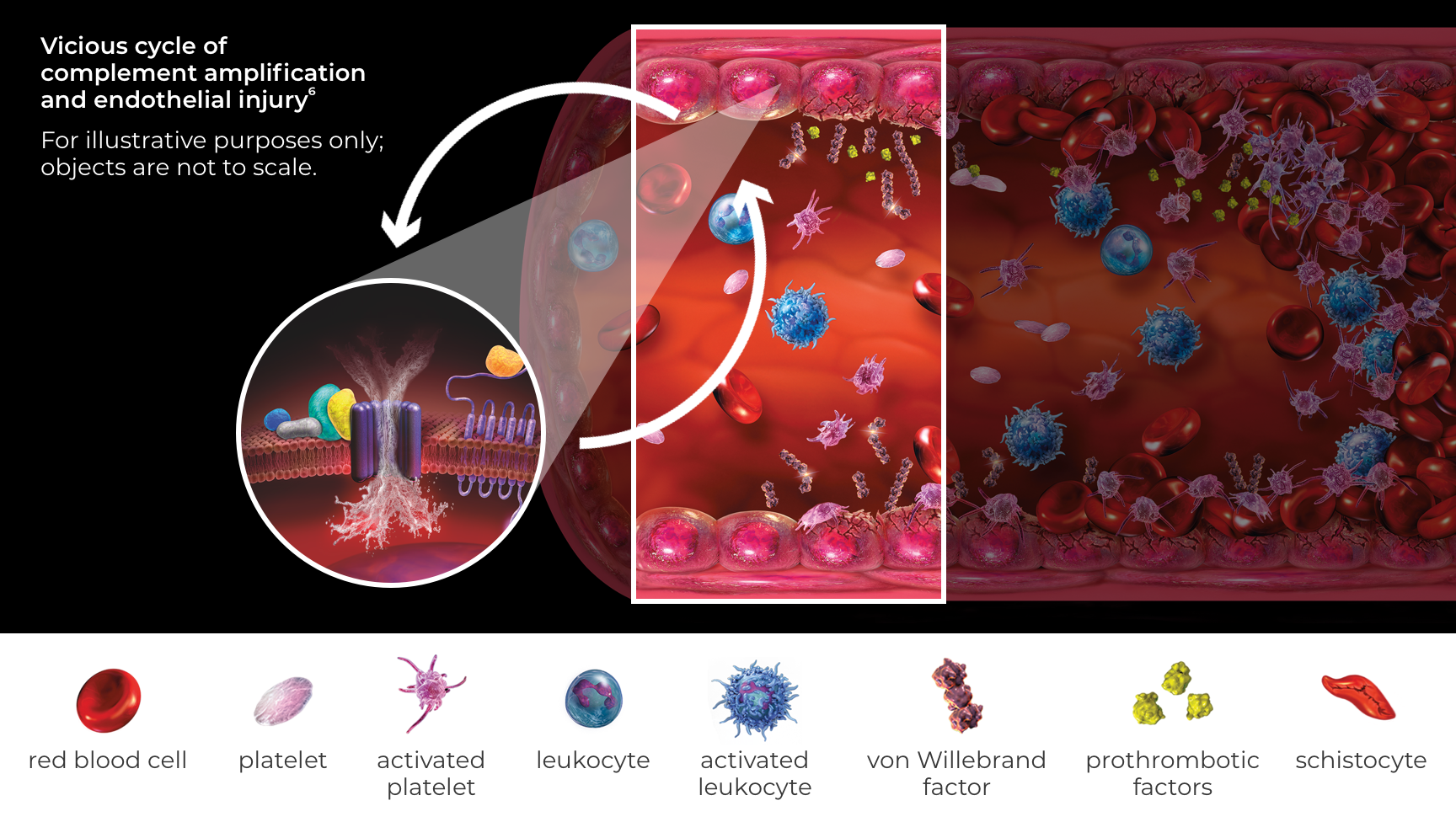
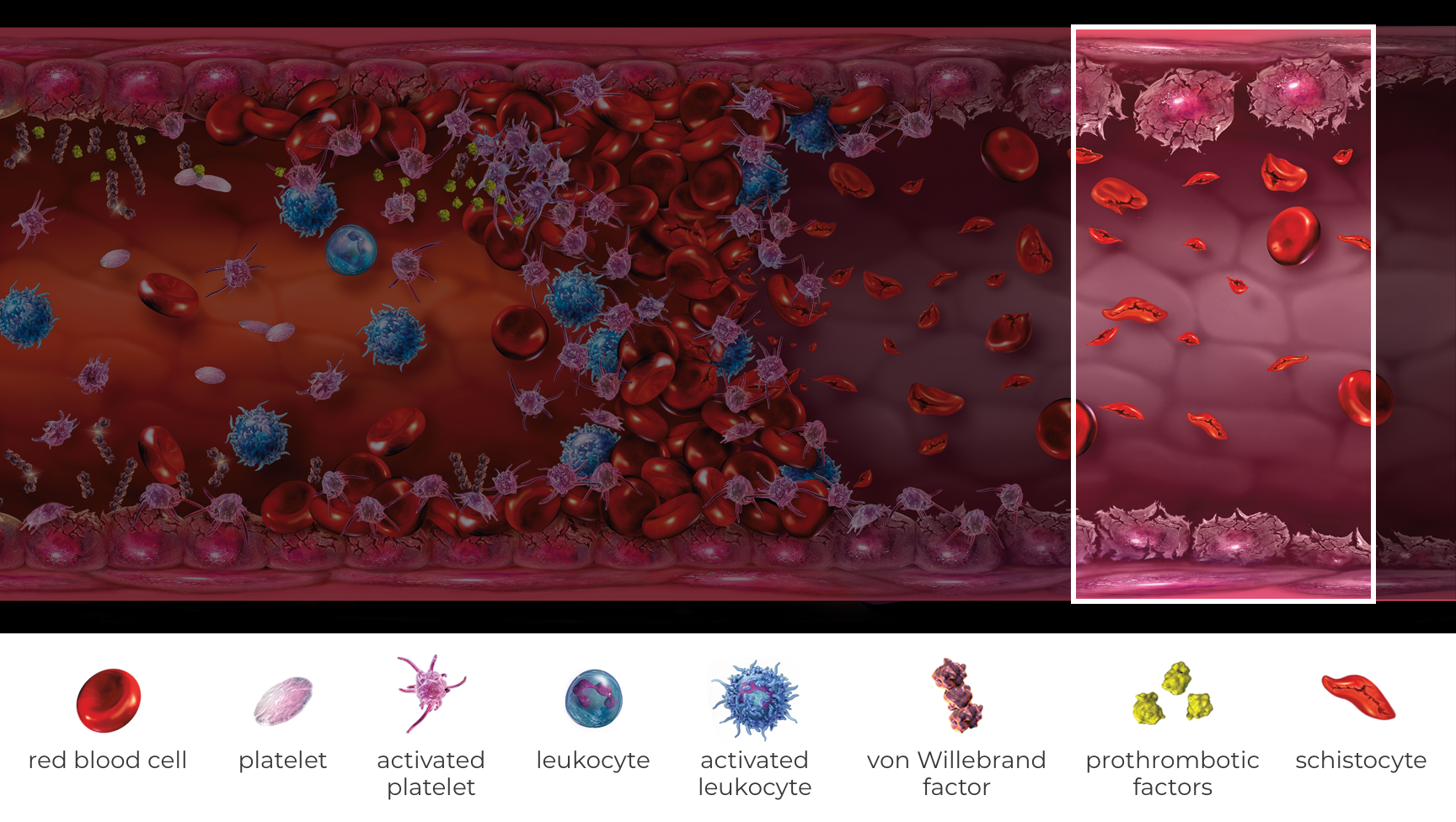
Review how TMA manifests in atypical-HUS and can lead to resulting organ damage.1
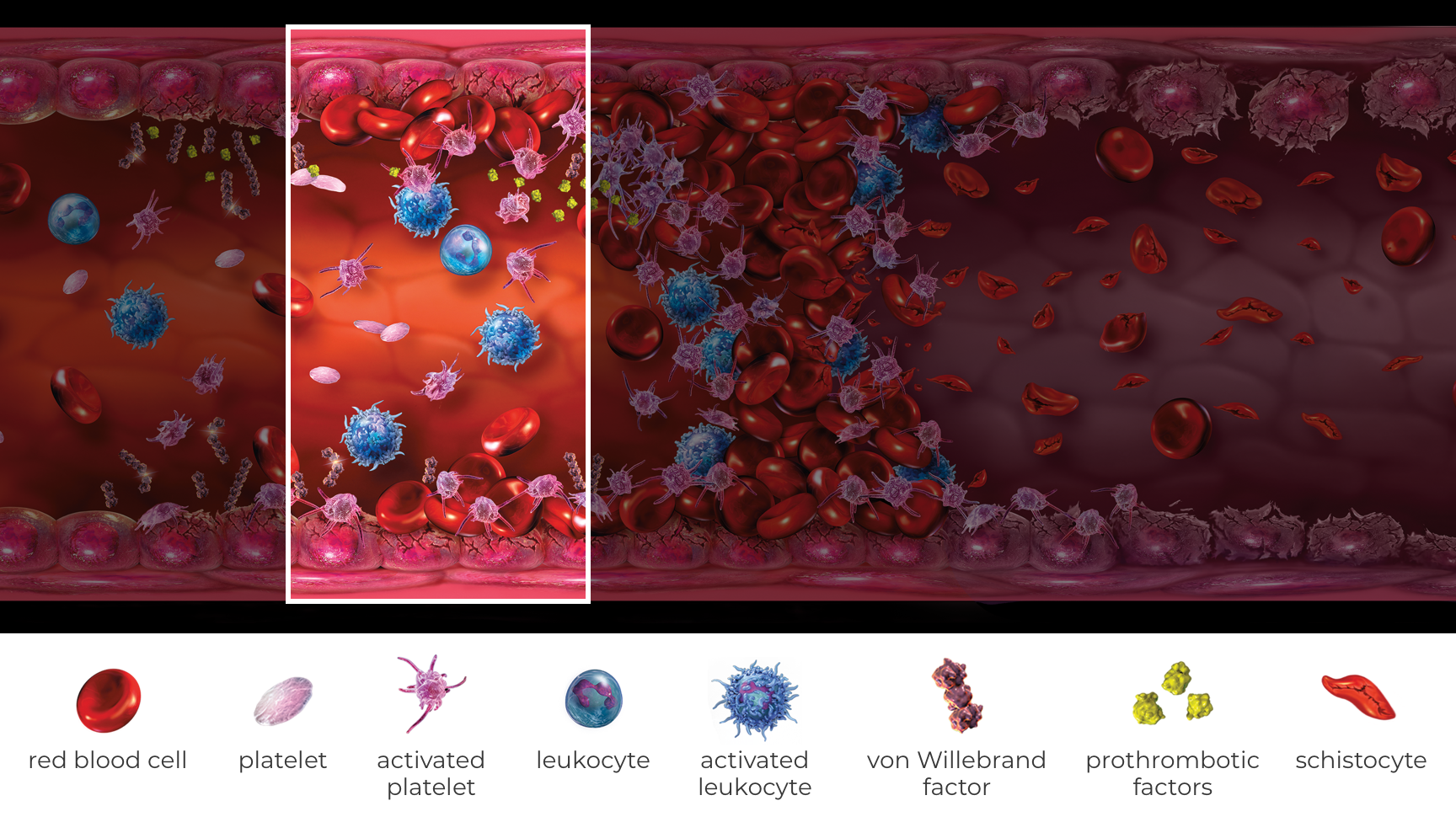
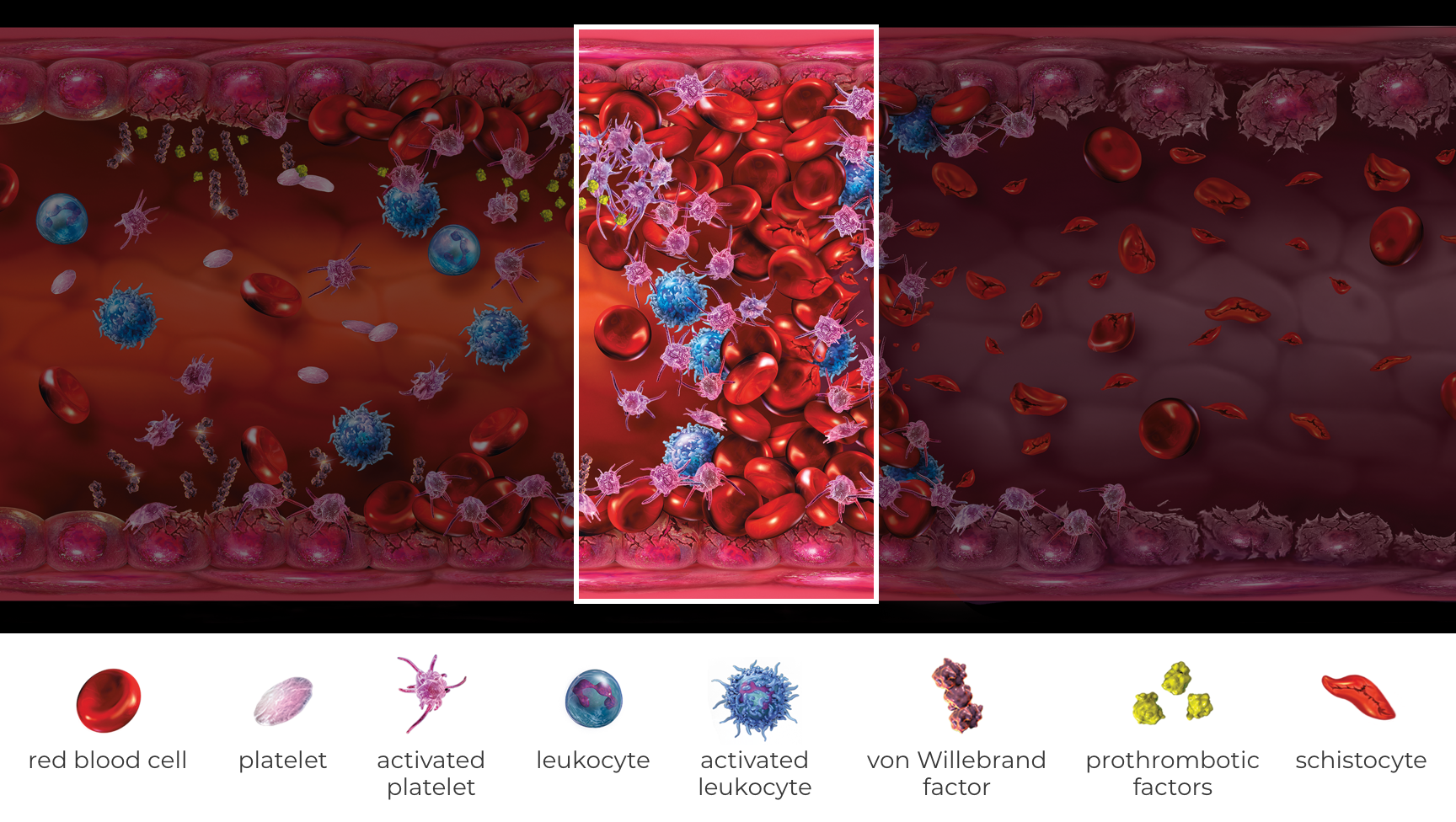
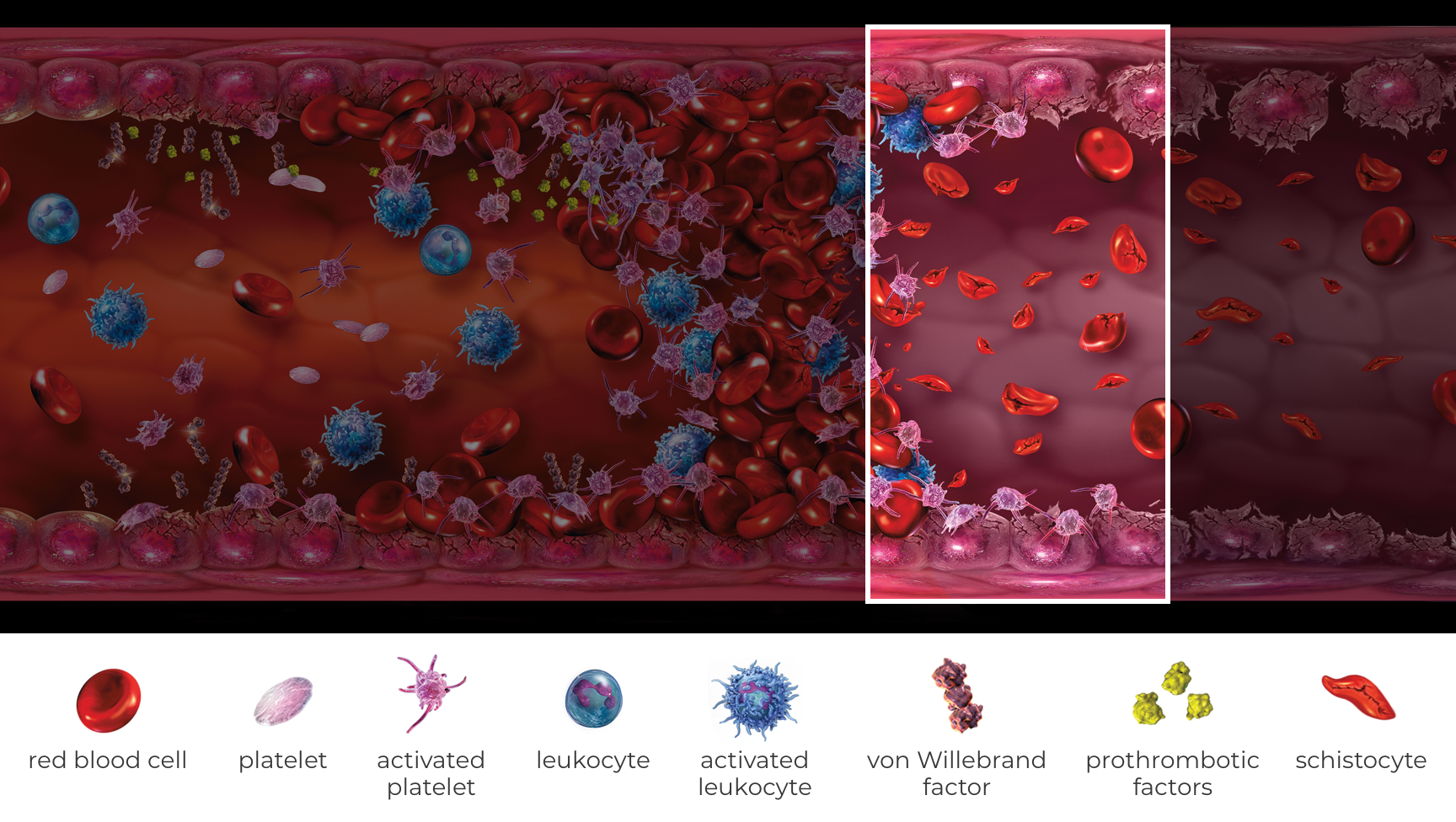
Scan through the cyclical stages of endothelial injury that result from TMA lesions to understand how irreversible tissue damage can progress.5,18,19
The assembly of multiple C5b-9 complexes on the surface of endothelial cells causes endothelial injury, leukocyte recruitment, and platelet activation.6,20-22
Binding of C5a to the C5a receptor results in a decrease in the endothelium’s anticomplement and antithrombogenic properties.6,21,24
Disrupted endothelial cells:
Biomarkers of complement activation, inflammation, endothelial cell activation and damage, coagulation, and renal damage (eg, Ba, sTNFR1, sVCAM-1, D-dimer, U-cystatin C) are similarly elevated among patients with atypical-HUS receiving or not receiving plasma exchange or plasma infusion.26
Ba=complement factor Ba; sTNFR1=soluble tumor necrosis factor receptor-1; sVCAM-1=soluble vascular cell adhesion molecule-1; U-cystatin C=urinary cystatin C.
Atypical-HUS patients can show involvement in more than 1 organ system.2,7,27-29*
*The organ-specific symptoms associated with atypical-HUS are reported from published literature and are not limited to those listed above.
eGFR=estimated glomerular filtration rate; ESRD=end-stage renal disease